We recently sat down with Andrea Williams from Milwaukee Radio Group. Gary Garland, WPA’s executive director, and Anna Warren, who lives with Parkinson’s, were featured.
Take a listen here:
We recently sat down with Andrea Williams from Milwaukee Radio Group. Gary Garland, WPA’s executive director, and Anna Warren, who lives with Parkinson’s, were featured.
Take a listen here:
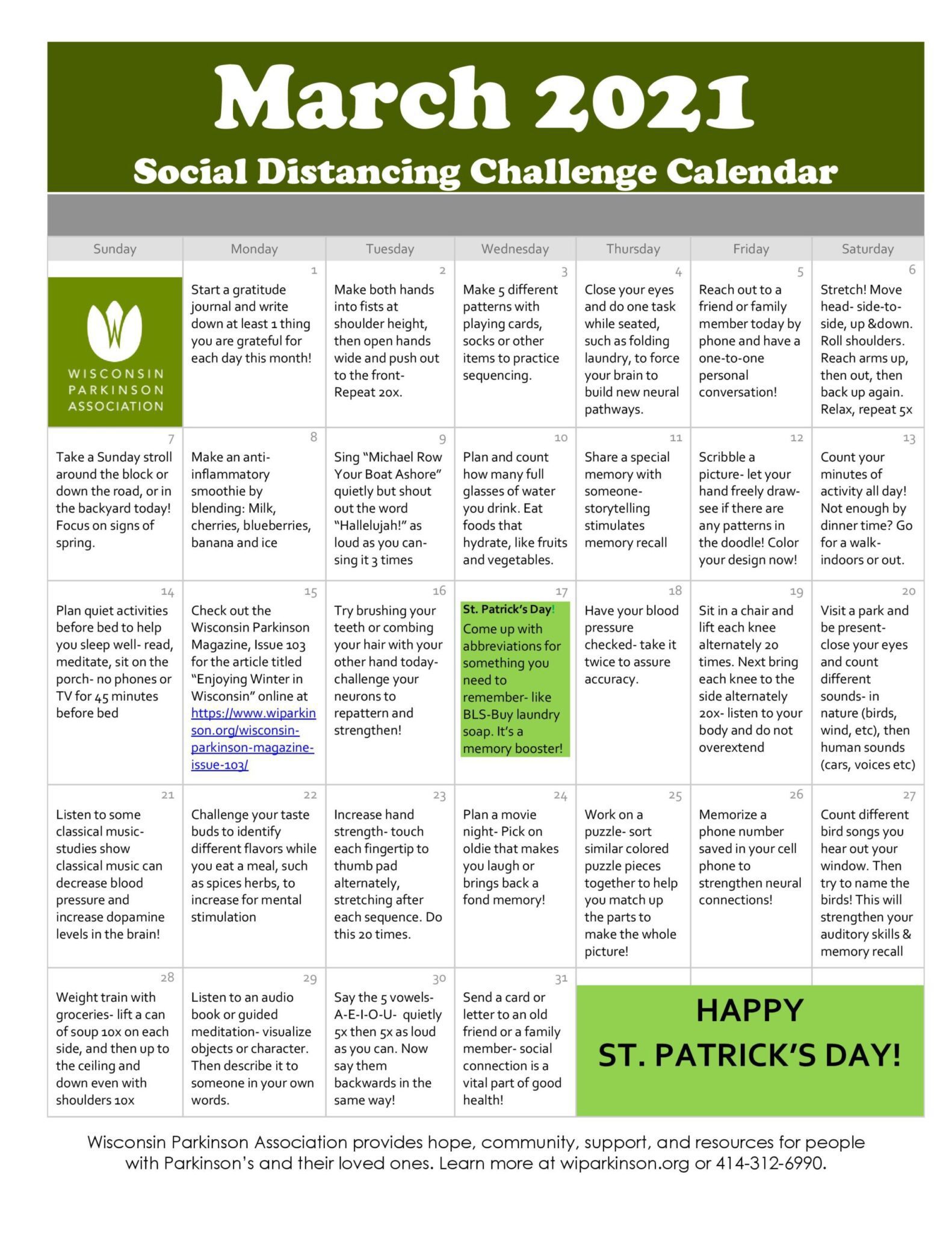
Check out this activity calendar to keep yourself active and engaged this month!
People with Parkinson’s disease experience more stress than those without this disease, and high stress levels associate with a worsening of symptoms, research based on a patient survey reported.
Mindfulness, a practice of maintaining a heightened state of awareness of thoughts and feelings, may help to lower stress in people with Parkinson’s, especially anxiety and depressive feelings, it also reported.
These findings were in the study “Stress and mindfulness in Parkinson’s disease – a survey in 5000 patients,” published in npj Parkinson’s Disease.
A team led by researchers in the Netherlands sent out a survey through The Michael J. Fox Foundation’s Fox Insight program. The survey asked a variety of questions about stress, Parkinson’s, and related factors.
Survey answers were returned by 5,000 patients and by 1,292 controls, mostly relatives, spouses, or friends of patients who did not have Parkinson’s. Patients’ mean age was 67.3, their average disease duration was 5.9 years, and 48.6% were women. Among controls, the mean age was 60.8 years, and 78.0% were women.
Most survey respondents (93%) were white, and most (82.6%) lived in the U.S. Of note, not all survey respondents answered every question; the researchers analyzed data that were available.
Analyses demonstrated that perceived stress was generally higher in people with Parkinson’s than in controls. This effect was also “much larger for men than for women,” the researchers wrote.
Parkinson’s patients also scored higher than controls on measurements of anxiety and depression, and lower on dispositional mindfulness (a trait that allows a person to be aware of the present moment, even during ordinary tasks). These differences were all independent of age or sex.
Among patients, higher stress scores associated with worse symptoms for all symptoms assessed (including sleeping problems, depression, involuntary movement, and slowness of movement.)
The symptom most affected by stress was tremor: 81.8% of patients reported a worsening in tremor during periods of stress.
“It should be noted, however, that PD [Parkinson’s disease] patients may perceive externally observable symptoms such as tremor more easily than slowness of movement or muscle stiffness, which could (partly) explain the difference between tremor and other motor symptoms,” the researchers wrote.
Patients who reported higher stress levels were also found to be more likely to report lower scores related to quality of life, self-compassion, and dispositional mindfulness. Stressed patients were also more likely to show high scores related to rumination (continuously thinking about the same thoughts, which are often sad or dark).
In free-text portions of the survey, patients commonly stated that stress worsened their cognitive and communication difficulties, and heightened emotional symptoms like anxiety.
Physical exercise was the most commonly reported stress-reducing strategy in the survey, mentioned by 83.1% of patients. Other frequent approaches to lessen stress included religion, music, art, reading, taking anti-anxiety or antidepressant medication, and looking for social support (e.g., talking to a friend).
Over a third (38.7%) of Parkinson’s patients reported practicing mindfulness — which involves focusing on the present moment, rather than fixating on the past or worrying about the future.
Of note, patients who were mindfulness users reported significantly higher dispositional mindfulness, and also higher perceptions of stress and anxiety. The researchers noted that it is difficult to tease out cause-and-effect relationships from this data. For example, people who are more stressed might be more likely to seek out mindfulness, or mindfulness practitioners may be more in touch with feelings of stress or anxiety and so recognize them to a greater degree.
Mindfulness also was associated with less severe symptoms across all motor and nonmotor symptoms measured.
“Patients perceived a positive effect of mindfulness on their symptoms,” the researchers wrote.
“Highest effects were seen for depression and anxiety, for which, respectively, 60.2% and 64.7% noticed improvement,” they added.
About half of mindfulness users (53.2%) practiced this technique once a week or more, while over a fifth (21.5%) practiced mindfulness once a month or less. Broadly, individuals who practiced mindfulness more frequently reported a greater easing of their symptoms, but consistent benefits were seen among all mindfulness users regardless of frequency.
The researchers speculated that, even when people aren’t actively practicing mindfulness, they may incorporate it into their lives more informally, through subtle changes to lifestyle or thought patterns.
These findings “[support] the idea that mindfulness is effective in reducing PD symptoms,” the researchers wrote, though they again noted they could not determine cause-and-effect from these data. Rather, “people for whom mindfulness is most effective might consequently practice it more.”
The researchers called for further studies, particularly in larger and more diverse groups, to better understand the effects of stress on Parkinson’s patients, as well as the potential benefits of practicing mindfulness.
“The significant beneficial effects that patients experienced from self-management strategies such as mindfulness and physical exercise encourages future trials into the clinical effects and underlying mechanisms of these therapies,” they concluded.
Check out this activity calendar to keep yourself active and engaged this month!
![]()
The World Parkinson Coalition is headed to Spain for the 6th World Parkinson Congress from June 7-10, 2022. In order to help prepare delegates who live with Parkinson’s or care for someone with Parkinson’s, they are launching the first ever WPC dual language webinar series in English and Spanish. Each topic covered is a topic that people with Parkinson’s have identified in survey data that they want or need more information to better understand and to be able to make more informed decisions around treatment options.
We want our community members to live their best possible lives, but also to be able to articulately speak about Parkinson’s. The more they know about this disease, the better they can explain their needs to their healthcare team and better educate their families and communities.
Each set of webinars will use bi-lingual Parkinson’s experts. These experts will present and take questions in two webinars back to back. The first webinar will be in English. Once this session ends, they will take a short break and then will give the same talk in Spanish. We believe that it’s important for people to hear about their disease and treatment options in their native language directly from the experts.
A new study of approximately 80,000 patients shows that people with Parkinson’s disease (PD) have a 30% higher risk of dying from COVID-19 than people without the neurodegenerative condition.
The new analysis conducted by researchers with University of Iowa Health Care based on patient data in the TriNetX COVID-19 research network suggests that Parkinson’s disease is an independent risk factor for dying from COVID-19.
The UI research team led by neurologists Qiang Zhang, MD, and Nandakumar Narayanan, MD, PhD, identified the COVID-19 patient cohort as of July 15 and analyzed the mortality data eight weeks later. They found that 5.5% (4,290 out of 78,355) of COVID-19 patients without PD died compared to 21.3% (148 of 694) COVID-19 patients who also had PD.
However, the patients with PD were generally older, more likely to be male, and less likely to be African American than the patients without PD. All of these factors also increase the risk of death from COVID-19. So, the UI team used two approaches to account for these differences: logistic regression with age, sex, and race as covariates, and matching each PD patient with five non-PD patients with the exact age, sex, and race, and performing a conditional logistic regression. In both cases, the researchers found that the risk of dying from COVID-19 was 30% higher for patients with PD. The findings are published in the journal Movement Disorders.
“We recognize the limitations of this study, it is retrospective data from a single database, but we are confident that these data show that Parkinson’s disease is independent risk factor for death in COVID-19,” says Narayanan, UI associate professor of neurology and a member of the Iowa Neuroscience Institute. “We believe this observation will be of interest to clinicians treating patients with Parkinson’s disease, and public health officials.”
The researchers say the findings should also inform patients with PD, and their physicians, of the increased importance of preventing COVID-19 infection in these patients.
“For our own patients, we can give advice that it’s important that you wear a mask. It’s important that you socially distance,” says Zhang, an associate in the UI Department of Neurology.
Zhang adds that physicians should also weigh the increased risk of death from COVID-19 when considering how to care for PD patients in person during the pandemic.
A potential reason why PD patients have an increased risk of death from COVID-19 may be related to the fact that COVID can cause pneumonia and pneumonia is a leading cause of death in patients with PD. This is partly because Parkinson’s patients can have trouble swallowing or choking that can cause aspiration.
“We are all focused on COVID right now, but this is a clear example of a respiratory illness that leads to increased mortality [in PD patients]. These findings may also have implications for understanding risks for PD patients from other diseases, including influenza,” Narayanan says. “I would recommend a flu vaccine and pneumonia vaccine to try to prevent these problems in patients with PD.”
In addition to Narayanan and Zhang, the UI research team included Jordan Schultz, PharmD, Georgina Aldridge, MD, PhD, and Jacob Simmering, PhD.
When someone you love is sick, it can cause stress and anxiety. Illness, especially Parkinson’s, can take a physical and emotional toll on caregivers and family, particularly when they are far away. For everyone dealing with a Parkinson’s diagnosis, there is generally worry and uncertainty.
Around 7 million people in the US today are caregivers; nearly 20 percent perform this role long distance. As baby boomers continue to age, the number of caregivers is projected to increase significantly in the coming years. Developing strategies to partner in caregiving can help families stay involved with the progression of treatments, and ease the varied burdens of a Parkinson’s diagnosis on families.
Caregiving describes the time and attention needed to care for relatives or friends when they require additional support caring for their own needs. Help provided can take different forms; it may include everyday tasks like grocery shopping, transportation, and meal preparation. It can also encompass managing medical appointments and household finances, and full-time personal care. Caregiving is generally unpaid, done out of love or sometimes a sense of obligation.
Caregivers can come from different places: a husband, wife, or partner, a child, parent, or sibling, other relatives, friends, even neighbors. Someone close to the patient is the most important non-medical member of the care team. Yet the fears and urgency of caring for someone so ill can take a physical, psychological, and financial toll on caregivers and their own families.
Caregivers often experience physical and psychological side effects when caring for a family member or friend. Studies have shown that those who provide informal, unpaid care to someone with significant limitations to their independence can experience a negative impact on their own health and personal lives.2 For example, some people don’t take the time to eat right and exercise; this may result in both weight gain and mood disturbances. Others may find they don’t have the time for a social life or to participate in their regular leisure activities.
Those who live far enough away that they are unable to have daily, face to face interactions with their relatives are known as long-distance caregivers. Caregiving can be more complex when distance, time, cost, and other factors limit accessibility. Factors like work, family, and transportation can affect the ability to sustainably provide care. Communications from long-distance caregivers can be occasional or regular, but for many, it is more just periodic checking in. Making a phone call to say hello and share updates about work, family, and life in general is an example of how long-distance touchpoints have value.2
Long-distance caregivers have support needs that may differ from nearby caregivers.2 They typically are not part of the medical team and thus have limited relationships with or access to the doctors involved in care and treatment of their loved one. Many report high stress and anxiety over the changing health status of their loved one.2
The impact on family dynamics can also be stressful when care is split between nearby and long-distance caregivers. If the primary caregiver is nearby they may feel that the family member or friend who is far away may be of less help, and not feel the same impact of the burden of caregiving. This can lead to resentment and disputes. Yet, studies have demonstrated that caregivers who are unable to see their family member regularly are stunned by physical and functional changes associated with treatments. This can result in experiencing more stress for the remote caregiver over the dramatic changes seen, due to lapses in time between visits. By comparison, for caregivers nearby, observed changes in a loved one undergoing treatments are more gradual.
There are steps long-distance caregivers can take to stay connected and participate in a more involved way. When someone you love is sick it can be upsetting and disruptive. Getting to know the medical team providing care, whether in the hospital, medical office or at home, can help you stay connected with medical updates and treatment decisions. Some people use technology to stay in touch. For example, FaceTime and Skype can be used for video chatting and offer a sense of being closer.2
Technology can also make it possible to be a part of medical appointments and treatment decision discussions. Try to arrange in advance for some kind of video conferencing technology with the medical team. That way you can listen to what the doctors have to say as well as ask questions.2
Research supports findings that long-distance caregivers do better personally when they participate in appointments via videoconference, get their own personal counseling time with social workers and improved access to medical information and caregiving resources.2
Long-distance caregivers who are heavily involved in caregiving estimate they spend at least one day a week managing the affairs of their loved one. They report missing work, having to rearrange their schedules, and other distractions when caring for someone far away.
Most importantly, remember to listen to your loved one, support them when making treatment decisions, and prioritize your own self-care. There may be distance between you and your loved one, but that doesn’t mean you can’t still support and care for them.
Dayne Beccano-Kelly shares his experience as a black professional working in Parkinson’s research, explains why visibility and education are the key to increasing diversity – and how unrepresentative studies and a lack of information are failing black people with Parkinson’s around the world
I describe my work as a researcher as like a telephone conversation that I’m listening into. For people with Parkinson’s, the line gets a bit faulty. I’m trying to see what causes the messages to change so that we can clean up the line.
I spend a lot of time in a lab here at Oxford University, however I do try to see individuals living with Parkinson’s, too. We have a Parkinson’s group doing outreach and funding. We also host Oxford Parkinson’s Disease Centre day, where we organise talks and bring together collaborators, independent scientists, carers and people with Parkinson’s. This always really puts what I’m doing into perspective.
As a researcher, it’s important to have a cold scientific approach so as not to be biased – but I think it’s vitally important to remember that while you cannot be completely emotionally driven, you must remember that the money we are spending is going towards finding something to help.
I’ve worked in two principalities across four different countries, and I’ve never encountered a senior black member of academic staff in neuroscience within my departments.
I’ve been told by professionals in my field that I was there because of positive discrimination. It’s very hard to be told that, but you have to remind yourself ‘no, that’s not true’. They looked at my skin colour before talking to me and decided that I must be in my position because of the colour of my skin. That’s racism.
I believe that there are two key things that you can do to promote BAME (black, Asian and minority ethnic) individuals in STEM (science, technology, engineering and mathematics): visibility and education. Telling students from an early age, ‘you are capable of getting there’. Raising the issue, talking to everybody in the room – not just the black students – and making them fully aware that you can begin to end the problem with your generation.
Disorders like ALS (amyotrophic lateral sclerosis), MS (multiple sclerosis) and essential tremors have all been shown to have different levels of prevalence and incidence – as well as a wide range of symptoms – within different ethnic groups. But there has not been enough research into how Parkinson’s affects individuals from different ethnic groups. While some studies suggest black individuals are less likely to get Parkinson’s than Caucasian western individuals, others may indicate it is equal.
There has been instances where it has been proven that in African and West Indian communities, individuals tend not to go to the doctors enquiring about Parkinson’s because they only experience non-motor symptoms. By not manifesting typical Parkinson’s features, they may be treated for something else, meaning it takes them longer to receive the treatment they really need.
In certain parts of the world, it’s common for black patients to not get as much time with doctors, and for their symptoms to be deemed milder than somebody of Caucasian descent. We need more global information about Parkinson’s in those underserved groups. It’s important for the black community that we’re informed enough to notice these non-motor symptoms and seek help.
Parkinson’s studies are biased towards people of Caucasian descent. We need to address that fact and keep pressing forward with recruiting more BAME individuals into the research. Parkinson’s organisations need to be a part of that – diversity needs to become normative.
We must see that there is a disparity in what researchers are sampling; check the ethnic groups present and break research down to realise that we can’t draw a conclusion because there are simply not enough black people.
Having more information will help us help people with Parkinson’s, and that means when they come to the doctor they won’t be turned away, not because of the colour of their skin, but because they don’t believe that they’re presenting symptoms in the way that they would expect.
There is this issue across the board with BAME treatment. Whether it be in the workplace or care, there needs to be acknowledgement coupled with action.
Dayne Beccano-Kelly is a career development fellow in Neurobiology at the Department of Physiology, Anatomy and Genetics, University of Oxford. He completed his undergraduate degree and PhD at the University of Leeds, UK, before undertaking postdoctoral research in Dundee, UK, and Vancouver, Canada. Article from Parkinsonslife.eu.
In this fast-paced world, staying connected can be difficult enough for seniors. Add in a pandemic for which people 65+ are most vulnerable, and you have a situation that can lead to intense feelings of isolation, loneliness and hopelessness. But through technology, seniors can stay connect in meaningful ways, such as:
Safely Accessing Resources
Whether due to physical limitations, weather or current events, sometimes it’s impossible for seniors to get out and explore their communities. This makes it important for older adults to be able to access a working home internet connection, both for purposes of socializing and for safety’s sake. Ideally, seniors should have access to both a senior-friendly device and a solid internet connection.
Electronics are increasingly senior-friendly, with both smartphones and tablets worth considering. Internet access can be a challenge, though.
For seniors living in more rural areas, Verizon’s home internet service can be a practical and affordable option for seniors, connecting them to one of the most reliable networks in the nation. With a powerful connection, seniors can access resources like support groups for Parkinson’s, or safely discuss issues with healthcare providers via telehealth appointments.
Regularly Checking In With Long-Distance Loved Ones
Being geographically separated from family can be especially burdensome for seniors. When travel for families is not an option, seniors can start feeling the effects of isolation and depression, both of which are growing issues within aging populations. Seniors may feel unloved, forgotten or without a sense of purpose when they are unable to connect with those they care about.
Thankfully, aging family members can reach out to long-distance family members via social media. Social media has become a sort of safe haven for senior mental health, but there may be times when seniors crave actual face time. As CNBC notes, video chat apps are increasingly useful for maintaining healthy connections.
Staying Safe, Comfortable and Secure While Aging in Place
When visiting with an aging family member is not possible or practical, aging in place tech can assist with staying abreast of well-being from afar.
For instance, a smart home security system that helps aging family members feel protected at home can double as a monitoring system for long-distance caregivers. Virtual assistants allow caregivers to check in with senior loved ones, plus they provide seniors with a sense of comfort. If a senior has mobility issues that makes moving around difficult or even dangerous, smart home options like automated lighting provide peace of mind.
Tech can be a priceless tool when it comes to protecting seniors and preserving their quality of life. Instead of feeling isolated, seniors can use tech to stay connected to the people they love.
In the latest in Parkinson’s Life’s ‘Ask the expert’ series, psychiatrist and neuroscientist Dr Philip Mosley explains how behavioural addictions can affect the lives of people with Parkinson’s – and shares how a recent study used a virtual casino to find out more about the condition.
That’s a complex question. From a biological standpoint, dopaminergic medication seems to act on the brains of people with Parkinson’s to bias risky decision-making and reinforce sensation-seeking behaviour, even if it comes at great personal cost.
As well as being involved in the regulation of movement, dopamine is an important ‘teaching signal’ in the brain that helps us to learn from negative and positive experiences, so that our future behaviour is ‘optimal’ for our environment.
The theory is that dopamine from Parkinson’s medication imbalances this signalling in certain regions of the brain and causes a ‘better than expected’ teaching signal – so that rewards are more rewarding and losses are less painful. Only some of the people who take dopaminergic medication develop these compulsive behaviours, so we believe there is something about the specific pattern of degeneration in the brains of those that do that makes them at higher risk.
If we can unravel why a problem occurs, or at least explain some of the variability, then we can deliver more accurate and personalised information to people with Parkinson’s who are making decisions about the risks and benefits of their treatment.
If we understand who is at higher risk, we can also develop personalised management plans that take into account this vulnerability profile – whether that be choice of drug, the timing of follow up, the provision of external psychological support and how much the family are involved in oversight of the treatment plan.
Common behaviours I talk to my patients about include pathological gambling, compulsive spending, binge eating, hypersexuality and becoming excessively involved in hobbies or pastimes to the exclusion of all other interests.
These behaviours can be absolutely devastating. I have met people who have gambled away their life savings, lost their marriage or been prosecuted for actions they have performed whilst under the influence of these medications. There is often an ethical quandary to navigate: people generally know their behaviour is ‘wrong’ but feel compelled to continue to act in this manner despite being intellectually aware of the potential ramifications.
Stigma prevents people from seeking help and acknowledging their difficulties, which only serves to prolong these problems and magnify the fallout. My personal approach is to encourage a non-judgemental atmosphere in which people feel comfortable enough to talk freely without fear of embarrassment.
The aim of our research was to understand more about why some people with Parkinson’s are vulnerable to developing these impulsive and compulsive behaviours. We hypothesised that brain structure, which varies between different people, was a key factor in determining whether or not compulsive behaviours would follow after people received dopaminergic medication.
We took a group of 57 people with Parkinson’s on dopaminergic medication and focused on two brain networks thought to be crucial for decision-making: a network for ‘choosing’ the best course of action and a network for ‘stopping’ inappropriate actions. We used an advanced method of brain imaging which allowed us to visualise the structure of connections between the different brain regions involved in these circuits.
Alongside the brain imaging, we created a virtual casino for our participants. We measured their level of impulsive behaviours through their tendency to place high bets, switch between slot machines and accept “double or nothing” gambles. We then compared behaviour in the virtual casino to the connectivity of the ‘choosing’ and ‘stopping’ networks, to see if there was an association.
The virtual casino was developed by a team of amazing collaborators at the Translational Neuromodeling Unit, in Zurich Switzerland, led by Professor Klaas Enno Stephan. Much of the research into impulsivity and compulsivity in people with Parkinson’s is carried out using pen-and-paper tests or else quite rarefied paradigms that don’t have much relevance to ‘real life’. We felt that our casino would simulate an environment with greater overlap and relevance to the problems experienced by our patients. In Australia, slot machines (known as ‘poker machines’ to Australians) are a huge public health concern with high levels of problem gambling throughout the community, and so it seemed appropriate to adopt this model.
For the most part, the greater the strength of the ‘choosing’ network and the weaker the strength of the ‘stopping’ network, the more impulsive participants were – that is, they had a greater tendency to behave recklessly in the casino environment by placing large bets, trying lots of different poker machines and making ‘double or nothing’ gambles.
Of our 57 participants, 17 developed clinically significant compulsive behaviours problems during clinical follow up. These participants could be differentiated when we examined the interaction of brain structure, medication dosage and betting behaviour in the virtual casino.
In other words, the real-world environment of the virtual casino, which simulated one aspect of compulsive behaviour, allowed us to unpick the relationship between brain structure and dopaminergic medication to identify those who developed behavioural addictions.
Compulsive participants expressed impulsive gambling behaviour in the virtual casino, as we would have predicted. However, their brain structures suggested they would be conservative (that is, they had a weaker ‘choosing’ network and a stronger ‘stopping’ network). The size of the dose of dopaminergic medication didn’t appear to influence reckless behaviour in these individuals. This suggests the neurodegeneration associated with Parkinson’s prompts a difference in the way the brain works in these people with addiction.
Don’t despair – you can recover from these problems. Talk to your neurologist, your family doctor, or a psychiatrist who knows about Parkinson’s. Recruit your family or close friends, if you can, as part of your support network, and draw on the experience of those in your local support groups, if you feel comfortable sharing some information about what you are going through.
Recent Comments